


Epilepsy and the brain.
Epilepsy is one of the most common neurological disorders, affecting roughly 50 million people around the world.
Researchers at Oxford are looking at how epilepsy can be prevented, diagnosed and treated.
Our experts are also raising awareness of the condition to reduce stigma and improve quality of life for people with epilepsy, particularly those in under-resourced communities.
Content warning:
Please be aware that this page refers to depression and topics such as suicide.
Tags:


What is epilepsy and what causes it?






What is epilepsy?
The word epilepsy derives from the Greek epilambanein, meaning ‘to seize’.
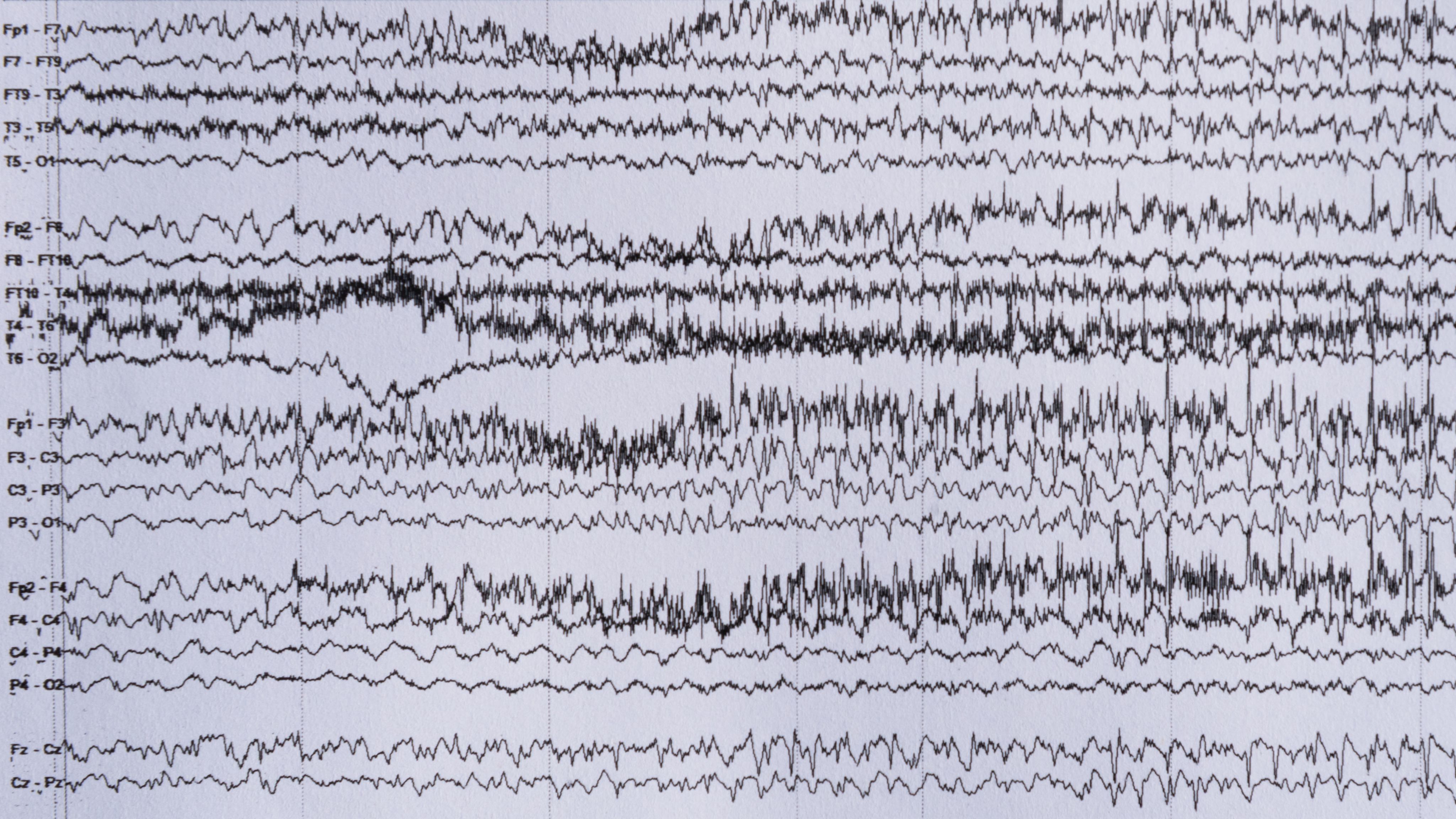
It is a condition characterised by seizures which involve episodic, abnormal activity in nerve cells in the brain.
50 million
people worldwide are affected by epilepsy
Epilepsy always involves seizures but the types and symptoms differ. When people have convulsive seizures, the body stiffens and shakes. With more subtle seizures, people may lose awareness for short periods of time.
As we get older, epilepsy becomes more common. It’s the third most common neurological disorder in people aged over 65, after stroke and dementia.
1 in 20
people will have a seizure at some point in their life. Around 1 in 130 people will develop epilepsy
The genetic causes of epilepsy.
Genetics may be causally linked to some types of epilepsy.
Understanding the mechanisms is key to developing targeted new treatments.
To tackle this, researchers Oxford contributed heavily to the 100,000 genomes project during the 2010s.
The project improved our understanding of conditions such as Otahara syndrome, a rare form of epilepsy.
It also improved our understanding of brain malformations in people experiencing seizures.
The project paved the way for a new Genomic Medicine Service in the NHS, which is enabling faster and more accurate diagnoses of genetic conditions and faster identification of the most impactful treatments.
Building on this today, the Genseize project, led by the Radcliffe Department of Medicine's Associate Professor Usha Kini, offers sophisticated genetic testing to epilepsy patients.
Using artificial intelligence, the team is also exploring how genetic epilepsy patients respond to treatment.
By better understanding the role of genetics in epilepsy, we can accelerate improved diagnostics and treatments.
Autoimmune epilepsy.
Autoimmune Epilepsy was a term coined in Oxford, and describes epilepsy caused by the body’s immune system.
Experts in the Nuffield Department of Clinical Neuroscience (NDCN)'s Autoimmune Neurology Group are researching the role of specific antibodies (LGI1, CASPR2, NMDA and GAD) in epilepsy.
These are proteins made by the immune system to tag viruses and bacteria, but sometimes mistakenly target the body’s own tissues, causing disease.
If we can better understand the ways in which antibodies cause certain types of seizure, we can develop more targeted treatments.
Understanding how epilepsy affects the brain.
To develop better treatments, we need to understand how functional networks in the brain respond and adapt to epilepsy and to underlying brain lesions that can cause it.
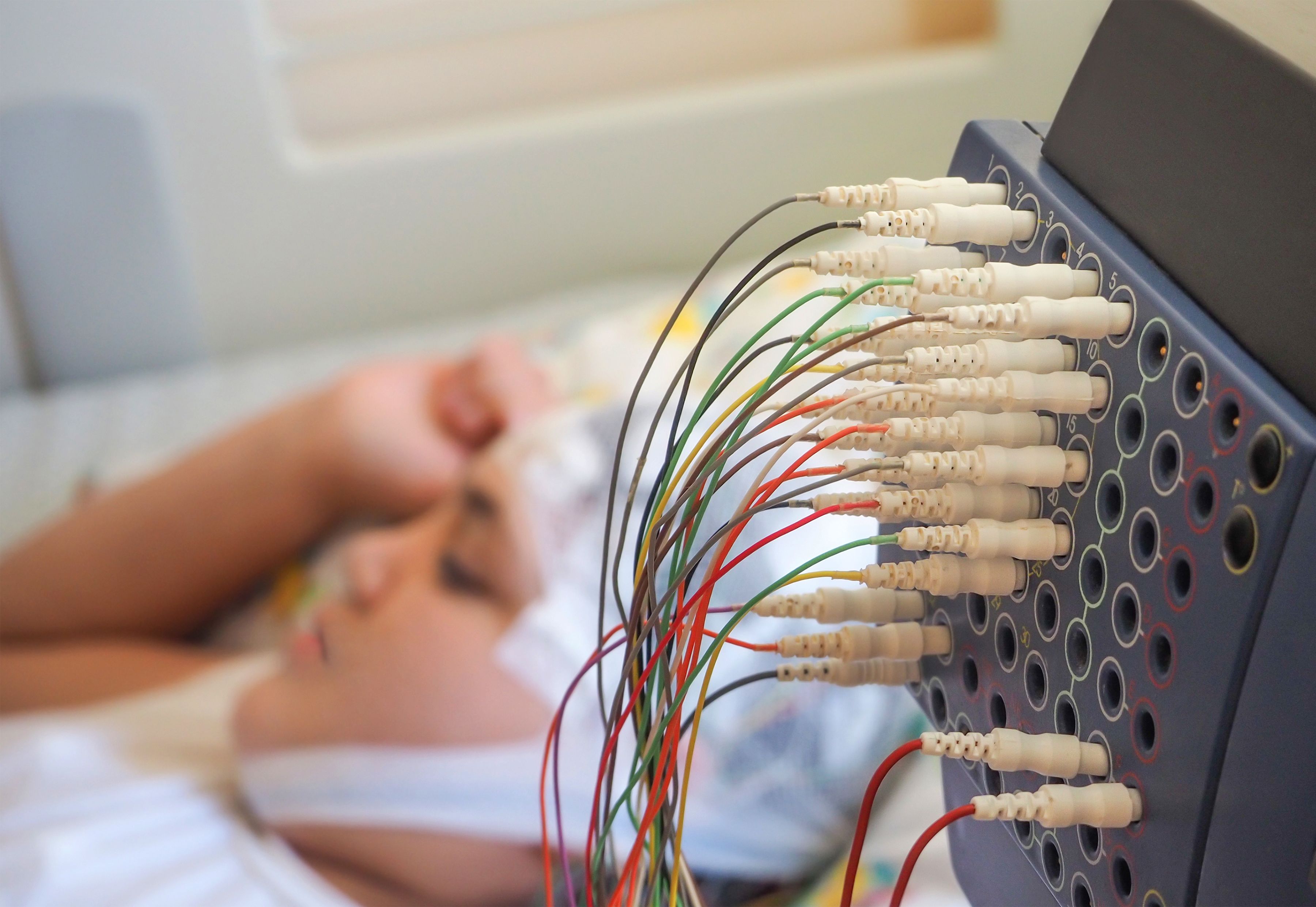
A key challenge is studying brain activity in people with epilepsy.
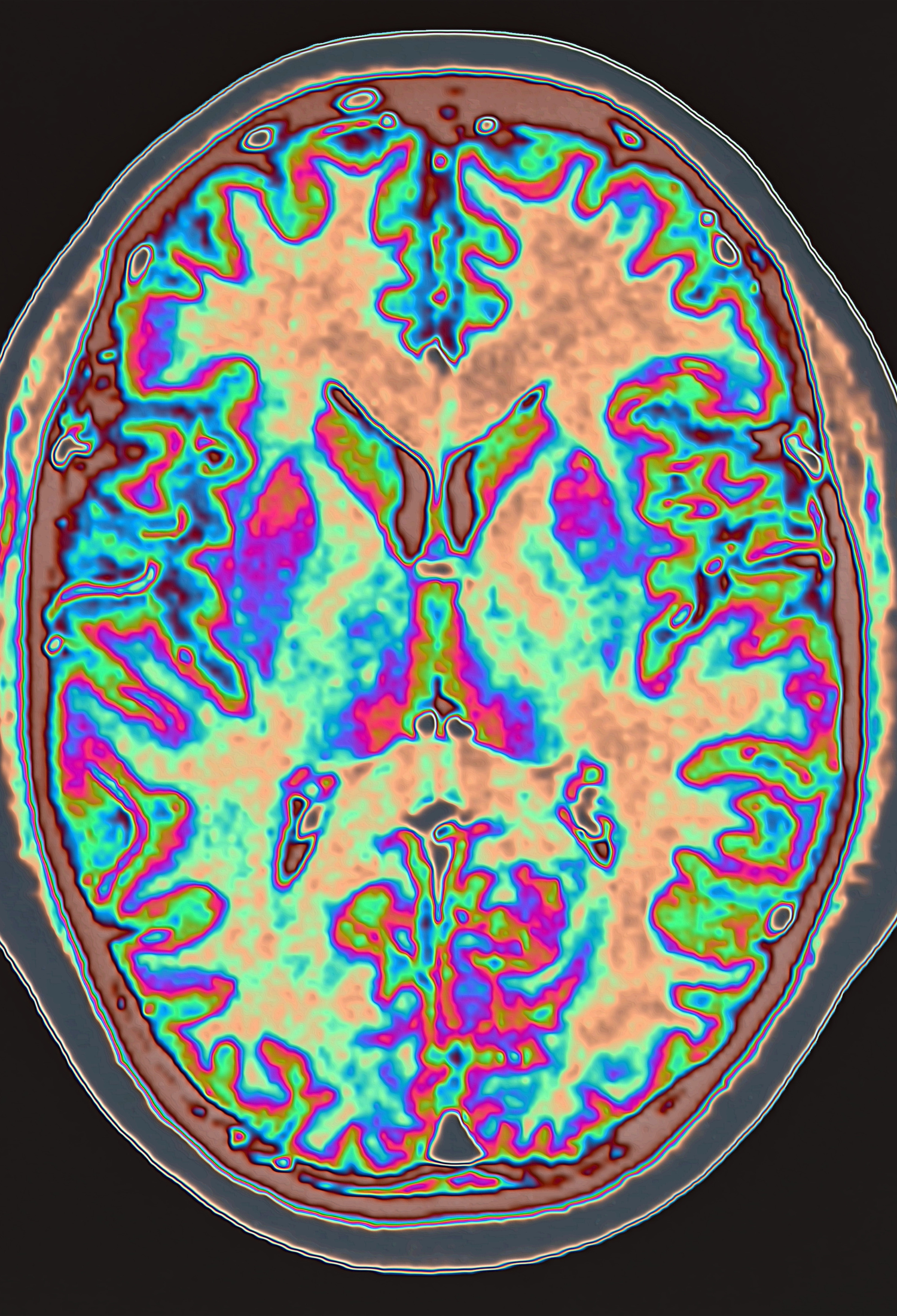
Oxford researchers are tackling this using state-of-the-art brain imaging methods, Functional Magnetic Resonance Imaging (fMRI) and Diffusion Tensor Imaging (DTI).
NDCN’s Associate Professor Natalie Voets’ and Dr Jane Adcock’s research focuses on understanding how functional systems in the brain, particularly those involved in memory, respond and adapt to acute and chronic brain injury.
This creates opportunities to observe epileptic brains.
For the small proportion of patient presented with a surgical option to reduce seizures, the decision can be difficult.
Complications of brain surgery can involve memory loss, and loss of other functions.
Oxford’s research aims to improve the selection of patients likely to benefit from surgical intervention, while minimising risks to functions central to their quality of life.
As we aim to improve our understanding of epileptic brains, we need to expand access to high quality brain imaging across demographics.
In order to improve our understanding of brain development in childhood, Oxford researchers, in collaboration with colleagues from the University of Nottingham and University College London, have helped to develop a wearable ‘bike helmet’-style brain scanner.
By measuring tiny magnetic fields generated by the activity of neurons in the brain the Optically Pumped Magnetometers (OPM-MEG) scanner reveals which areas are active during specific tasks. It also records data millisecond-by-millisecond, meaning it can track neural oscillation (or ‘brain waves’) in real time.
Unlike conventional scanners, which require patients to lie still, the new device is wearable and works even if people move their heads.
This makes it easier to scan participants with epilepsy who find it hard to stay still, such as children or those with co-morbidities like Parkinson’s or dementia.
In June 2025, the latest version of the Optically Pumped Magnetometers (OPM-MEG) brain scanner was installed at the Oxford Centre for Human Brain Activity (OHBA).
Co-morbidities and epilepsy-related conditions.

Links to mental illnesses and early deaths.
Epilepsy can affect more than just seizures.
Co-morbidity is where the condition occurs alongside other issues such as physical or psychological disorders or diseases.
This can reduce the quality and length of life in people with epilepsy, and is something that has historically been underexplored.
10 times
People with epilepsy are 10 times more likely to die before their mid-fifties compared with the general population
In 2013, Oxford led a first-of-its-kind study to examine links between mental illness and early death in people with epilepsy.
Researchers, including Professor Seena Fazel and Professor Charles Newton, studied the health data of almost 70,000 people with epilepsy born in Sweden across a 41-year window.
They compared data to participants’ unaffected siblings.
They found that people with epilepsy were four times more likely to have received a psychiatric diagnosis compared with the general population.
They were also four times more likely to die by suicide, and there was a strong correlation with mental illness and substance abuse, suggesting a need for treatment liaison between clinical epilepsy services and psychiatric and addiction services.
A 2023 Oxford-led meta-analysis further explored mortality risk factors in the general population, this time looking at studies covering over 117 million patients from around the world.
They found that people with epilepsy were twice as likely to die from suicide, furthering the call for holistic approaches to epilepsy treatments.
‘Although it is well-recognised that psychiatric and addiction disorders occur in epilepsy, in high-income Western countries, epilepsy is often managed by neurologists only. The findings from this study would suggest that clinical epilepsy services should review their liaison with psychiatric and addiction services as a priority.’
Treating Alzheimer's with epilepsy medication.
Alzheimer’s affects around 800,000 people in the UK alone and costs almost £23 billion per year.
Like people with epilepsy, Alzheimer’s patients experience seizures more often, which contribute to the loss of nerve cells.
They may also experience abnormal brainwave activity without an obvious seizure, which can disrupt thinking and memory. Oxford researchers are therefore exploring ways an epilepsy drug can help people with Alzheimer’s disease.
The anti-epileptic drug Levetiracetam can reduce abnormal brainwave activity and reverse memory deficits in a mouse model of Alzheimer’s disease.
In 2020, the Nuffield Department of Clinical Neuroscience (NDCN)'s Professor Arjune Sen led the ILiAD pilot study (Investigation of Levetiracetam in Alzheimer's Disease).
Although curtailed by the COVID-19 pandemic, the trial demonstrated that Levetiracetam was well tolerated in this potentially vulnerable group.
Further research is now proposed, with a larger sample group, to assess potential memory benefits.
COVID-19 and epilepsy.
COVID-19 posed new risks for epilepsy patients and their healthcare workers. Oxford researchers undertook initial rapid studies, and follow-up research, to identify the key factors affecting health outcomes.
In 2020, Professor Arjune Sen led a global survey to assess the risks COVID-19 posed to epilepsy patients, their carers, and healthcare workers. The study became one of the largest of its kind, receiving almost 4,000 responses. UK respondents reported changes in seizure frequency, mental health, and sleep.
The study highlighted the need for proactive healthcare services to help epilepsy patients mitigate risks.
20%
of clinicians felt less confident in diagnosing epilepsy following the pandemic shift to remote consultations
The pandemic forced many healthcare consultations to shift online.
A separate study, led by Professor Sen and Professor Charles Newton, sought to understand how this impacted clinicians' wellbeing and their ability to provide adequate epilepsy care.
According to 70% of respondents, most of their consultations had become remote. As a result, a fifth of respondents felt significantly less confident in diagnosing epilepsy.
There was also a notable impact on healthcare workers’ mental health during the pandemic, with 43% reporting an impact.
The study concluded that health services need to be redesigned to address the risks associated with remote delivery, to ensure optimal outcomes for people with epilepsy and their clinicians.
55%
People who had COVID-19 were 55% more likely to develop epilepsy or seizures over the next six months than people who had influenza in an Oxford study
Questions remained about the link between COVID-19 and epilepsy or seizures, however. Two Oxford studies have tackled this problem.
In the first, researchers looked at health records of people who had been infected with COVID-19 and carefully matched them with a group of people who had been infected with influenza.
Each group consisted of 152,754 people, none of whom had previously been diagnosed with epilepsy or recurrent seizures.
The team compared the incidence of epilepsy and seizures between the two groups over a six-month period following the initial infection. They found that the rate of new cases of epilepsy or seizures was 0.94% in the people who had COVID-19, compared with 0.6% in those who had influenza.
The results suggest that people who had COVID-19 were 55% more likely to develop epilepsy or seizures over the next six months than people who had influenza.
The risk was particularly high in children, with the study highlighting the importance of preventing infections in young populations.
A subsequent 2022 analysis of 89 million patients' healthcare records found that SARS-CoV-2 infection increased the risk of epilepsy and premature death.
Collectively, these findings show the need for further research to develop better healthcare pathways for people with epilepsy and associated conditions.



Improving epilepsy treatments.



Improving access to anti-seizure medication.
There are a range of drugs used to manage epilepsy.
However, accessing this medication can be particularly challenging in lower-income countries.
Professor Arjune Sen gave expert consultation for a 2024 WHO report on these issues, evaluating barriers such as fragmented supply chains, affordability constraints and procurement limitations that restrict access to essential neurological medicines.
By using epilepsy as a worked example, the report demonstrates how addressing treatment access for one condition can strengthen planning and delivery across wider mind-brain health services, particularly in low-resource health systems.
This built on prior work by Oxford to expand fair access to the drug levetiracetam, a widely used and well-tolerated anti-seizure medicine that can deliver meaningful benefits for patients.
But in low-resource settings, getting consistent access is hard. To address this, researchers from the Centre for Global Epilepsy led the application that resulted in levetiracetam being added to the WHO Model List of Essential Medicines in June 2023.
This is a key step toward making the medication more consistently available, affordable, and normalised in epilepsy care.
Researchers from the Oxford Martin School are developing a digital tool to support more effective and holistic delivery of essential medicines worldwide, including epilepsy treatments.
The 'Medication Availability Tracking Tool’ uses real-time data and AI-powered forecasting to help health teams understand where medicines are located and where they are needed.
It is designed to work in settings where digital infrastructure is limited, and to support local decision-making without adding complexity.
With adaptability and open-source design at its core, the tool is intended to scale beyond its pilot setting in Zimbabwe.
Vagus Nerve Stimulation (VNS) Therapy.
Some patients have a drug-resistant form of epilepsy, while others may have conflicting health conditions which make medication unsuitable.
Technological treatments are being developed to fill this gap.
For example, Vagus Nerve Stimulation (VNS) Therapy, which involves intermittently stimulating the vagus nerve with electrical impulses. It aims to help regulate brain activity and reduce seizures.
1 in 3
nearly a third of patients have drug-resistant epilepsy
A long-term clinical study supported by Oxford’s Epilepsy Research Group has confirmed the effectiveness of this a neuromodulatory treatment for severe focal seizures in both children and adults with drug-resistant epilepsy and demonstrated the therapy's lasting impact.
The CORE-VNS study evaluated the outcomes of more than 800 people with epilepsy around the world who had been treated with VNS Therapy, produced by the US medical technology company LivaNova.
The three-year study was the largest of its kind, with Oxford University Hospitals (OUH) being the largest recruiter.
Deep Brain Stimulation (DBS) Therapy.
Deep Brain Stimulation (DBS) is a treatment involving surgery to insert a small device which stimulates specific parts of the brain.
While DBS treatments can be effective in reducing seizures in adults, treating children has been harder.
Children would outgrow implant methods, devices were limited to static stimulation patterns, and the batteries had to be surgically replaced every 3-5 years.
In 2024, the UK’s first trial of DBS for children with epilepsy began, in collaboration with experts from Oxford’s Department of Engineering Science.
The rechargeable device is mounted onto the skull and is attached to electrodes deep in the brain to reduce seizure activity.
The new cranial mounting overcomes previous issues of childhood growth, and the battery uses non-invasive induction charging to recharge.
The device also has the capacity to schedule therapy at different times of the day or night and to sense any seizure activity developing in the brain and respond with an appropriate dose of stimulation to halt its progression.
‘Our mission is to design pioneering research systems for exploring the treatment of intractable health conditions such as paediatric epilepsy. Oran is the first child in the world to receive this device and we are extremely pleased that it has had such a positive benefit for him and his family.’
The first UK patient was Oran Knowlson, then aged 12. He had been having severe epileptic seizures for eight years and often needed resuscitation.
Since having the device implanted, Oran has seen an 80% reduction in daytime epilepsy seizures, which had previously sometimes occurred hundreds of times a day and required frequent hospitalisation.
The CADET pilot project (Children’s Adaptive Deep brain stimulation for Epilepsy Trial) was award-winning, and will recruit three additional patients in this phase before 22 patients take part in the full trial.
Global epilepsy.


Epilepsy in low- and middle-income countries.
Over 85% of people with epilepsy live in low- and middle-income countries, where the increased risk from seizures contributes to much higher mortality.
Underfunding, limited access to medical care, and stigma towards people with epilepsy means that in some places fewer than 20% of those who need anti-seizure medications receive them.
Improving epilepsy diagnosis and treatment across Sub-Saharan Africa.
Epilepsy is particularly widespread in sub-Saharan Africa.
In part, this is due to preventable factors, which account for at least 25% of cases. But barriers include lack of diagnosis and appropriate treatments.
These can be compounded by enduring social stigma, which can make it hard for Africans with epilepsy to get jobs, form relationships or feel valued.
A coalition of organisations led by Oxford researchers created the Epilepsy Pathway Innovation in Africa (EpInA) project to tackle these challenges.
The primary EpInA study ran from 2019-2024 across Accra, Nairobi, Kilifi, and Mahenge.
Diagnostics on the go.
Research from the EpInA group has led to the development and validation of a diagnostic tool for convulsive epilepsy in sub-Saharan Africa, which has been implemented into a free app for healthcare workers in Kenya, Ghana and Tanzania.
Identification of convulsive epilepsy in sub-Saharan Africa is complicated due to a lack of resource and infrastructure. Using machine learning techniques, EpInA researchers developed and tested a region-specific questionnaire panel and predictive model to identify people who had experienced a convulsive seizure.
‘It is a privilege to be able to perform this work which we hope will make meaningful and sustained improvements in the care of people with epilepsy in Africa.’
The Epilepsy Diagnostic Companion is simple and accessible for health-care workers, does not require specialist knowledge to administer, and can be iteratively updated.
An initial finding from the Kenyan branch of the project was a high prevalence of epilepsy in the two urban informal settlements studied in Nairobi.
Non-convulsive epilepsy accounted for around one-third of observed cases. These findings are being used by local authorities and partners to inform policy and healthcare programming. Further analysis from across the project is underway.
With primary healthcare workers across sub-Saharan Africa now able to diagnose convulsive epilepsy with high accuracy, the app could lead to earlier, more accurate diagnosis of seizures, streamline referral pathways and improve care for people with epilepsy across the continent.
Training healthcare professionals to train their peers.
Care of people with epilepsy in Sub-Saharan Africa is hampered by a lack of healthcare staff trained to manage epilepsy.
EPInA provided initial training in the World Health Organization’s Mental Health Gap Action Programme (mhGAP) guidelines for the management of epilepsy.
In February 2025, Oxford and partners helped to deliver a week of coordinated training in Harare, reaching 104 healthcare professionals.
The Epilepsy Training in Adult Medicine (ETAM) course aims to equip healthcare professionals with essential knowledge and skills to improve adult epilepsy care. Two ETAM courses provided practical, case-based education in epilepsy diagnosis and management for clinicians working in resource-limited settings.
A Train-the-Trainer programme equipped 17 Zimbabwean clinicians with skills in adult education and facilitation. Local faculty independently led and delivered the second ETAM course.
Researchers from the Centre for Global Epilepsy, based at Wolfson College, also launched the first Solving Stigma in Epilepsy course, developed by the Faculty of History’s Professor Sloan Mahone, which explored clinical, cultural and historical dimensions of stigma.


Participants in the Solving Stigma in Epilepsy Course at the University of Zimbabwe
Participants in the Solving Stigma in Epilepsy Course at the University of Zimbabwe
The interdisciplinary UK-based team includes Associate Professor Sloan Mahone from the Faculty of History, Dr Guillaume Pages from the Oxford Martin School, Sonia Vallentin and Dr Gabriel Davis Jones, both from the Nuffield Department of Clinical Neurosciences, and colleagues from University College London, Newcastle University and London School of Economics.
Along with research teams based in Ghana, Kenya and Tanzania, the project is partnered with the World Health Organization, the Documentary Institute in Eastern Africa and the International League Against Epilepsy.

Some of the EpInA research team
Some of the EpInA research team
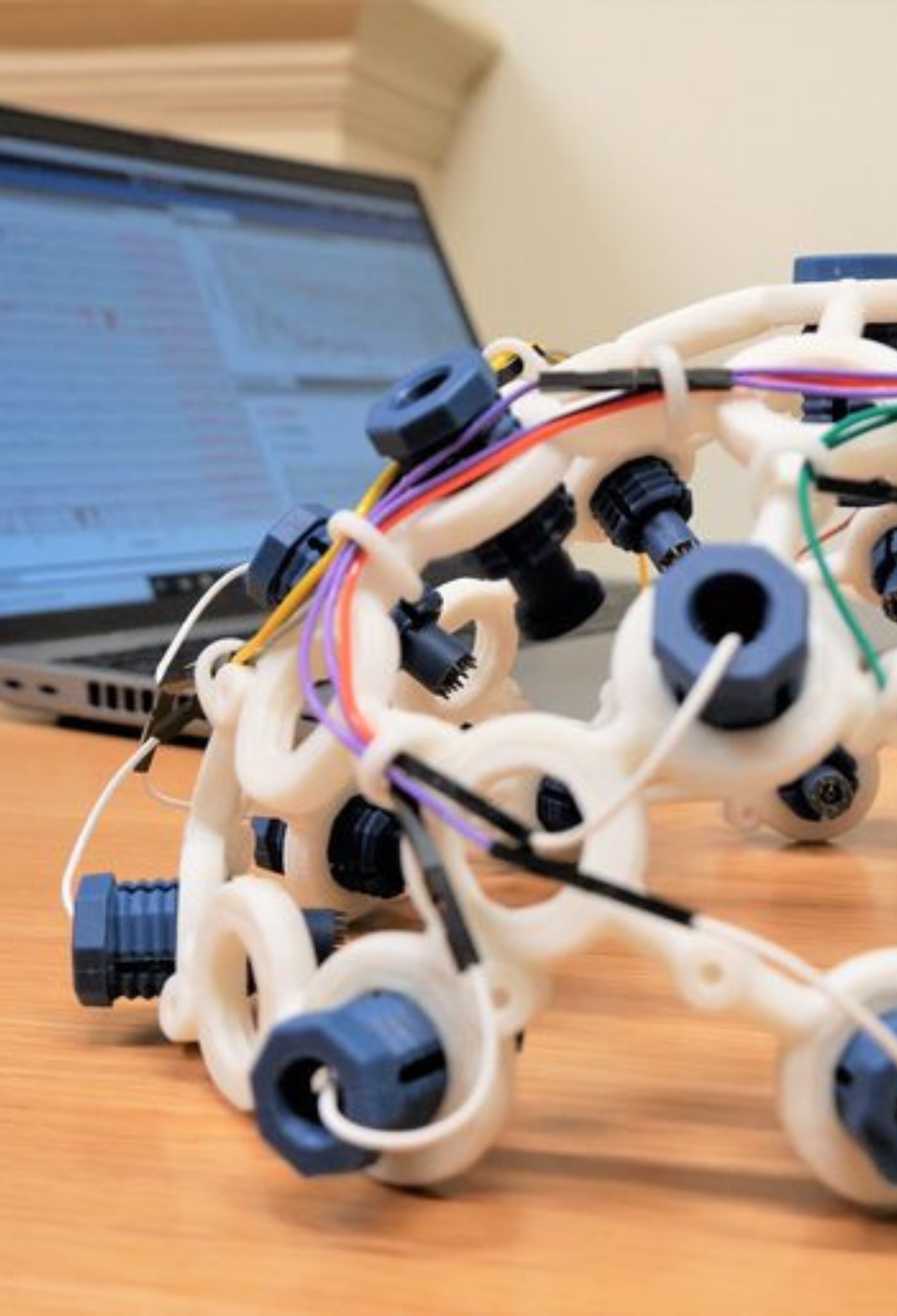
A close-up of the electroencephalogram (EEG) prototype. Image: EpInA
A close-up of the electroencephalogram (EEG) prototype. Image: EpInA

Participants with epilepsy and their partners completing a survey for a study in Zimbabwe. Image: EpInA
Participants with epilepsy and their partners completing a survey for a study in Zimbabwe. Image: EpInA

Professor Arjune Sen
Professor Arjune Sen
Portable EEGs in Zimbabwe.
Zimbabwe has a population of approximately 15 million, of whom about 10 million live in rural settings.
There are only six EEG machines in the country, most are in the capital city of Harare, and until a few years ago there was only one resident neurologist.
In rural Zimbabwe and similar places around the world, improving the understanding of epilepsy amongst regional health practitioners will ease gaps in the diagnostic pathway.
Improving access to EEG machines would also reduce a major barrier to diagnosis.
‘When I landed in Zimbabwe a few years ago, I doubled the number of neurologists in the country.’
The Oxford Martin Programme on Global Epilepsy is working to develop a wireless, lightweight and portable EEG that can be placed directly onto the patient’s head without needing pastes and the gluing of electrodes.
The results of the EEG are streamed directly into a decision-support app on a mobile phone or tablet, without the need for heavy-duty computing systems or an amplifier.
Researchers have already developed a prototype of this portable EEG system which is currently being field-tested by collaborators in Kenya, South Africa and India.
The results will be compared against the gold-standard hospital EEG and, if all continues positively, they will begin the rollout to rural communities.
A crucial step will be ensuring the portable EEG is affordable to manufacture and deploy because one of the greatest barriers to medical treatment in resource-poor settings is cost.
Associate Professor Sloan Mahone discusses the importance of listening to the lived experience of people with epilepsy
SMS reminders to improve health outcomes.
Poor adherence to medication regimes also reduces health outcomes in countries like Zimbabwe.
The EpInA project conducted a randomised controlled trial of SMS reminders (mobile text messages) to improve adherence.
Destigmatising epilepsy in Zimbabwe and understanding links with stroke.
Thanks to advances in healthcare and other factors, the number of older people in Zimbabwe has risen sharply in recent years. But as we pass the age of 50, disorders of the mind and brain become more common, including memory difficulties (dementia), strokes, and recurring seizures (epilepsy).
In Africa, seizures are deeply stigmatised, especially among older people. The stigma, and other health implications of epilepsy, reduce quality of life. It’s essential that, as more people live longer, they can do with health and dignity.
The ZEST study (Zimbabwean Epilepsy Stroke and demenTia) combines community-led workshops, focus groups and oral histories with clinical research.
‘We always set the highest standards and try to exceed them. The final part of our flagship ZEST programme will be to establish a centre for mind brain health in Zimbabwe.’
It aims to understand lived experience, stigma and risk factors. ZEST will follow people after stroke and those with later-onset epilepsy, using improved diagnostic technologies and testing practical interventions.
Findings will help strengthen care pathways with partners including the Ministry of Health in Zimbabwe and WHO.


Healthcare practitioners working with epilepsy patients in Zimbabwe, as part of the ZEST study led by Professor Arjune Sen
Healthcare practitioners working with epilepsy patients in Zimbabwe, as part of the ZEST study led by Professor Arjune Sen
Epilepsy research at Oxford and beyond.
The Oxford Martin Programme on Global Epilepsy aims to find solutions to improve diagnosis, understand and mitigate the social impact of epilepsy, and begin to build a better future for people with the condition – especially those in resource-poor settings.
The programme is closely aligned with the EpInA project, and the interdisciplinary Oxford team includes Associate Professor Arjune Sen, Professor Charles Newton, Professor Timothy Denison, Associate Professor Sloan Mahone, Sonia Vallentin, Dr Gabriel Davis Jones, Dr Guillaume Pages, Ines Pont Sanchis and Lisa Aissaoui.
The programme’s partner teams in Brazil, India, Kenya, South Africa and Zimbabwe connect researchers with communities and bring their own contextual expertise to the programme.
With a bold vision of a world where epilepsy is as manageable a disease as asthma, the programme has three aims:
- To understand the life experiences of people with epilepsy, the impact of epilepsy on communities, the nature of social stigma and perceptions of new healthcare technologies.
- To bring together engineers, medics and computer programmers to prototype and deploy portable high-density brainwave recording (EEG) to improve diagnostic accuracy.
- To use the local understanding gained from oral histories to create a suite of apps that will help support healthcare workers throughout the epilepsy diagnosis, management and follow-up pathway.
The Oxford Epilepsy Research Group, part of the Nuffield Department of Clinical Neurosciences, brings together researchers and clinicians from across the University of Oxford and Oxford University Hospitals to focus on all aspects of clinical and experimental epileptology, with an emphasis on clinically relevant research.
The group is led by Associate Professor Arjune Sen, also from the Nuffield Department of Clinical Neurosciences, and focuses on individual and holistic approaches to advancing care for people with epilepsy, who often face addition cognitive, psychological and psychosocial difficulties.
The researchers capitalise on the clinical expertise available at the John Radcliffe Hospital and the wider basic scientific research performed within the University of Oxford, collaborating with academic colleagues from universities across the United Kingdom, Africa, Australia, Brazil, Europe, India and the United States of America.
The group’s Clinical Epileptology team run a busy epilepsy surgery centre and contribute to EpiCARE: a European Reference Network for people with rare and complex epilepsies. They also work closely with epilepsy charities, particularly SUDEP Action and Epilepsy Society, and are part of the Humanology Project.
More from PULSE

